Brittany Jeffery
Edited & Additional Maps by Veronica Maisch

My recent abortion experience was 24 hours. After realizing why coffee had suddenly started tasting like salt, I called the NYC Health + Hospitals hotline, who set up an appointment for me at the hospital down the street. The next day I walked there — a true 15-minute neighborhood — and was offered choices of possible procedures to terminate my pregnancy. My safety, comfort, and convenience were prioritized, all for a neat copay of $13.36.
DOBBS
I chose surgical abortion, and although it was briefly painful, having to listen to Taylor Swift — throughout — was the worst part. It is because I exercised my right to health care that I’m able to sit here today and write these words. I remain in school, gung-ho about urban planning and progressing towards careerdom, now unburdened by the physical and emotional stress of life-changing care responsibilities. However, this is a sad story. As I grew older, I realized that my body entered the public domain and its reproduction is a process with a dizzying amount of stakeholders.
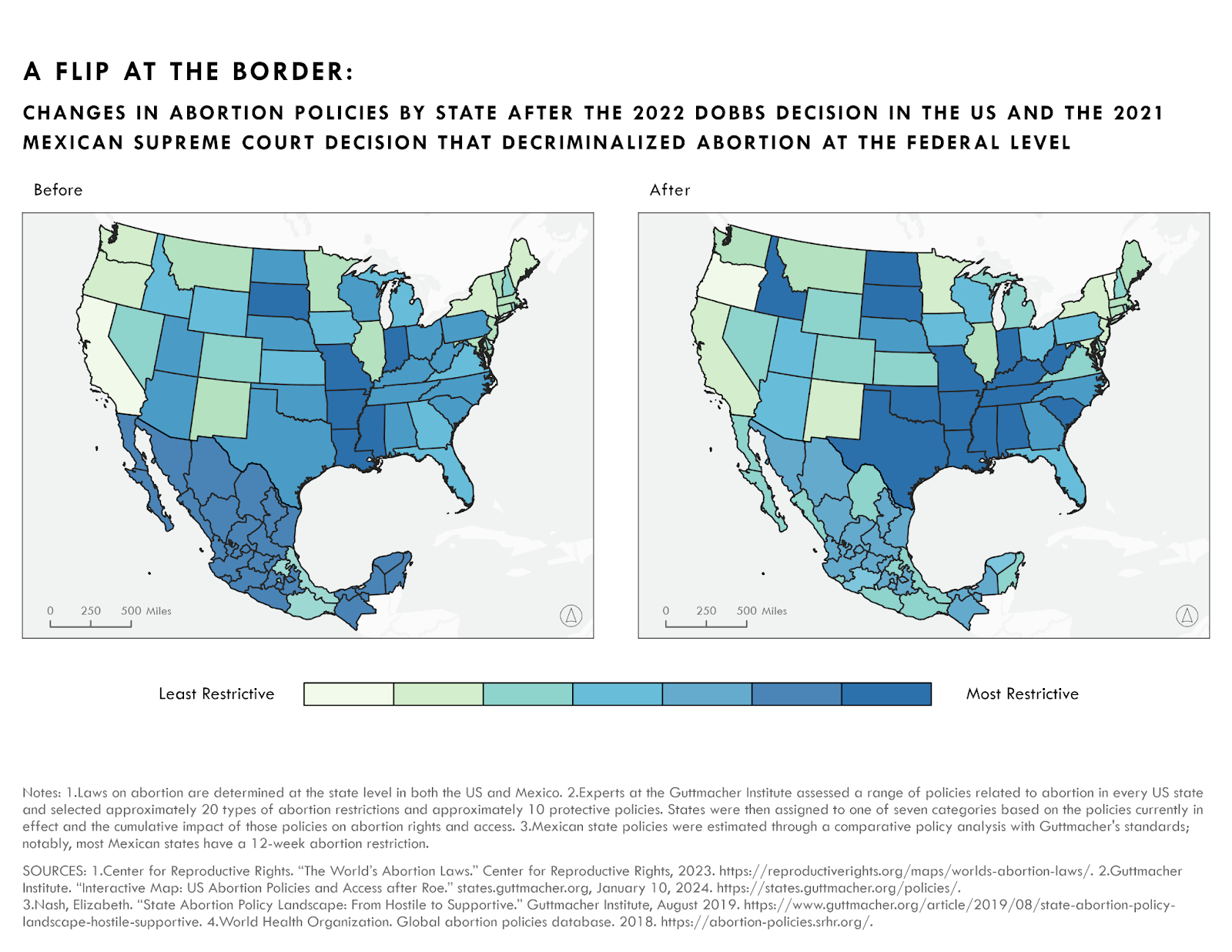
In the Dobbs decision, a Supreme Court ruling a year and a half ago, the right to an abortion was upended for millions who now face the consequences of extremist bans, frightening laws, and a fundamental desire to punish sexuality through litigation and imprisonment, trials and fines, lawyers and media attention, all with the stroke of a pen. Abortion care is being denied to previously eligible patients, obstetric care is receding in red states, and threats percolate, particularly in Texas, where a bounty law turns the public on each other. Horror stories from Ohio and Texas affirm what activists have been saying: this decision will only bring more suffering. The feminist glass facade of the US, once an ostensible global leader in women’s rights, has fallen.
GEOGRAPHIES
Planners and policymakers have long found it a pillar of their practice to justify interventions by showing the public why we need interventions — opportunities to thrive are not equally geospatially distributed. Mapping “abortion deserts” illuminates the bifurcated abortion healthcare landscape in the United States; in Texas, if you live close to El Paso, you may only need to drive half an hour to New Mexico to procure a safe abortion, while in Dallas, that drive could multiply to 8+ hours to a clinic.

As travel time increases, medication abortion becomes more critical. Data source: (JAMA Network) and additional analysis here.
Transportation planners have shifted their paradigms from mobility to access, which is fundamental to understanding this reality — the undue burdens of distance and cost in procuring an abortion become an insurmountable barrier for low-income people, who already face significant challenges in healthcare access. Even when abortion was legal, the obstacle course of getting one in many states became so onerous that your right to your own healthcare decisions was based on your zip code and financial security, a reality anathema to the best of the American promises of life and liberty.
Planners and policymakers, who face a world rife with inequity, are morally obligated to take into account the unsanctioned activities happening in their communities. We are frequently limited by borders in the field — city limits, razor fences, and ruler-straight lines all ignore physical and human geographical landscapes. Zooming out and looking at the subfield of regionalism is perhaps more apropos to this issue, as a patchwork network of care emerges. Anzaldúa and Keating may say it best: “Bridges are thresholds to other realities, archetypal, primal symbols of shifting consciousness. They are passageways, conduits, and connectors that connote transitioning, crossing borders, and changing perspectives. Bridges span liminal spaces between worlds.”
Abortion travel (which the right has hilariously taken to calling “abortion trafficking”) across state and national lines has become a necessity, offering paths to care if you can afford to get where you need to go. In a country where car ownership now averages 1k a month, with few public alternatives, these bridges to care become lifelines. An explosion in abortion infrastructure, including the growth of medical abortion, has created transnational networks that provide financial, emotional, legal, and health services. Combined, this exists as an invisible web of solidarity that has activists learning new languages, dodging rapidly changing restrictions, and coalescing mutual aid — away from the eyes and ears of states looking to flex political power. The infrastructure of pills tucked inside decoys, encrypted instructions bouncing through cell towers, and whispers between friends operates subterranean to the circling sharks of politically-motivated prosecutors looking to use people as examples.

Map Description: The Hyde Amendment (preventing federal funds from being used for abortion care) and the failure to expand Medicaid coverage in states like Texas, which have a huge childbearing population, compound barriers to care.
The Deep-South-sized hole in abortion access in the US is compounded by the radical legal and regulatory framework to prevent patients from accessing these procedures; prosecutors have become frighteningly creative in their ways of punishing abortion care recipients.
HEALTHCARE
Prior to Dobbs, over 50% of abortions were handled by a medication regime due to price, convenience, and the untraceable nature of these drugs. Two pills, mifepristone and misoprostol, safely terminate a pregnancy, with misoprostol being effective — but more painful — alone. (It’s unsurprising that mifepristone is constantly legally challenged worldwide, as it lessens the painful side effects of the procedure and is used only as an abortifacient, unlike misoprostol, which has many uses).
Mifepristone stops a pregnancy from continuing, and Misoprostol causes the uterus to expel its contents. These pills are essential, especially in a country with sky-high, racialized gaps in rates of maternal mortality. This is important to point out because, in states where abortions are restricted, there are sometimes exceptions “if the woman’s life is at risk” — an obnoxiously vague statement, as medicine operates in a constellation of gray areas that defer to a provider’s judgment — but carrying a pregnancy to term as opposed to an abortion procedure is well-established to be riskier to health and well being.
The American people, long fed up with for-profit ownership of healthcare and the high costs of our abysmal outcomes, have ventured abroad for decades for procedures and examples of what it could be in a world where UnitedHealth wasn’t worth 342.2 billion. A system laden with iatrogenic, and frankly, bad, care is being questioned, as increased agency on the part of patients feels like it’s percolating to other aspects of care. Recently, regulators approved over-the-counter birth control without a prescription, representing a shift in trusting women to make their own reproductive decisions on their own terms, with medical counseling offered on an as-needed basis.
Most of the history of abortion healthcare exists outside of formal systems, and the precursors to modern methods were radically developed from experimentation and laypeople trying desperately to take control of their own circumstances. The Berkeley Women’s Health Clinic popularized a procedure known as menstrual extraction that can be performed by laypersons, and the Jane Collective wrested control from physician exploitation by learning how to perform surgical abortions on their own. Critically, these procedures were safe in an era of the tropes of hangers and “back alley abortion.”
I asked my doctor 10,000 questions before my procedure, and the nurse held my hand as she walked me to the operating room, my little hospital socks slipping on the cold floor. But many others lack that aspect of emotional care, let alone access to a provider whom they can trust during the painful procedure. Many healthcare providers have distrusted, discriminated against, and deprioritized pregnant patients (disproportionately harming patients of color), leading to an erosion of the provider-patient relationship that should be based on the foundation of “do no harm.”
Healthcare providers, even when they aren’t mandated to report abortions, have chosen to inform police officers, putting their patients at risk. With these legal risks, it is a rational choice for many patients to step outside of the healthcare apparatus for services. Patients can incur debilitating costs, transportation obstacles, a dangerous lack of anonymity, and harassment from protestors. Providers who fail to account for these externalities operate in a framework that ignores the “whole patient.” Healthcare, like planning, should be grounded in the realities of the place, as the embodied geography of what the patient’s body is subjected to outside the exam room is paramount in making healthcare decisions.
The healthcare landscape for providers is plummeting already with the proliferation of private equity’s MBAs slithering into exam rooms. States are also punishing doctors with TRAP laws (Targeted Restrictions on Abortion Providers), contributing to a climate of fear in both practicing medicine and talking to your doctor honestly. Undue energy is being spent on onerous laws now that Dobbs has granted deeply misogynistic elements of local control to flourish. In pursuit of their own choices, more and more people are intentionally creating distance between themselves and red crosses, white coats, and novel-length itemized medical bills.
I do not seek to disparage all healthcare providers nor to undercut the critical roles that many of them play in the milieu of reproductive care access, advocacy, policymaking, and direct action for the best interests of their patients. Doctors have given their lives for reproductive rights in Kansas, performed late-term abortions in Colorado under sustained threat, and spearheaded a truly global service of shipping abortion pills from the Netherlands. In these cases, healthcare providers’ actions in the face of sustained worldwide opposition to reproductive health have been heroic. Before the kind of care they provide existed, millions died in the process of carrying a pregnancy to term. Untold numbers remain at risk of being forced into unwanted pregnancies or unsafe abortions in this new landscape, even if new networks of care continue to emerge through a patchwork of programs. Continuing to operate and practice reproductive medicine in such a tenuous state is a radical act of bravery. However, with the proliferation of self-managed abortions, robust data reiterating its safety, and the growing barriers to abortion care, it’s imperative that we ensure this affordable procedure is offered, with medical support, on an as-needed basis. The US is no outlier in draconian abortion policy, and the need is high in places still working towards a fairer existence for half of their population.
BORDERLANDS
The ubiquity of medication abortion has unlocked a new flip of the border whose fuzziness has long shaped the destinies of the US and Mexico. Mexico seems to have crossed us, trudging forward on a path we’re now receding backward on by decriminalizing abortion nationwide in 2023, although stigma remains. This hard-fought victory followed the example of other Latin American countries — many still deeply entrenched in anti-choice religions’ tentacles- in relaxing their stance in the face of changing public opinion. Direct actions persuaded the federal judiciary to quell discontent, as the US did in 1973 in the face of a growing feminist movement. Court victories can be a barometer of majority public opinion and a powerful tool — in the US, eons of racial progress have been buttressed by court decisions. However, this lever of our imperfect democracy was targeted with a long-term stratagem by the Christian right to overturn “settled precedent.”
Map description: Trends worldwide suggest increasing liberalization of attitudes towards abortion healthcare.
When abortion was illegal, Mexican women traveled to the Southwestern states for care, and this flow of patients and services has flip-flopped several times. Policy decisions made by politicians thousands of miles away geographically are clearly worlds apart ideologically, as people seeking abortions work around changing restrictions to get their needs met. The elastic US-Mexico border has retained significant bidirectional flows for generations, as products and peoples have traversed back and forth in search of opportunities and services. The US has been re-choked by theological rule, but Mexico’s liberation presents the possibility of a win within a religious framework, and all eyes look toward the next US election as a barometer of public opinion. In the meantime, Mexico’s proximity to Texas has become a well of water in the abortion desert.
An organization called Las Libres, based in conservative Guanajuato, Mexico, was the only one I found offering completely free abortion pills to ship to patients — a fact I discovered during my stress-filled Google search the minute I found out, a lump still in my throat from the shock. Las Libres (Spanish: The Free Ones), a reproductive health nonprofit run by Mexican women, has seen a surge in demand for their services since Dobbs. Their organization makes up a key piece of abortion care infrastructure, especially with pills being free and the concept of accompaniment, in which patients are provided with a trusted digital guide for the process of taking the pills. (Note: most abortion care providers reference sliding scale payments or available financial assistance for their services, but this adds a layer of bureaucratic difficulty). We see this trend in other issues in planning and policy — if the state ends or criminalizes a service, the burden shifts onto vulnerable communities and informal networks to meet the needs of a population abandoned or oppressed by the state’s policies.
DISCOURSE
Ideally, abortions would be easily accessible, on-demand, worldwide, but in absentia, nonprofits providing abortion services normalize them and change attitudes that can eventually form coalitions to push for an expansion of rights. Decentralized, patient-to-patient support networks and providers online plug holes in care gaps, building another bridge in the abortion infrastructure. Research is being done on the safety and efficacy of methods, and organizations, activists, and even comedians are bringing this formerly-taboo experience into the public discourse. The abortion landscape pulsates with every story told of every person who’s faced consequences from regulations or stigma coercing their decision-making. Every voice speaking out, however corny it sounds, makes the world a better place. Attorney Generals and courts overturning physicians’ decisions are all images that leave a profound disillusionment for the intertwined medical-legal systems regulating bodies and lives. Similarly risky medical procedures are performed with a banal numbness, to the point that mentioning your colonoscopy is a great way to get only some sympathy/disgust from coworkers, yet abortion is laden with so much cultural baggage projected onto you by others, ignoring how you feel. Even in writing this, I have a twinge of fear that telling this story may lead to consequences in future employment and social ostracization or judgment from family, friends, and peers.
FUTURES
Many fundamental policy changes cannot be predicted; the Pope’s home country legalizing abortion was not on anyone’s 2020 bingo card. There are signs of progress – every state with abortion access on the ballot has affirmed its support for it, as is the trend worldwide. In the American South, barriers were erected prior to Dobbs that polluted care for those most in need. Now that it has intensified into a ban, the frog and boiling water strategy of restrictions may prove to be a poison pill. Many ignored the gradual chipping away of abortion rights, but antediluvian bans with so-called medical “exceptions” and appalling case studies of the prosecution that have emerged post-Dobbs have radicalized many, including myself. While many states have enacted comically evil sets of restrictions, a few (shout out to Oregon) have deepened their support to produce some of the most liberal policies in the world. This path dependency also emerges in planning; areas that are densifying continue on that trajectory, while those decentralizing continue their endless sprawl. But history tells us that coalition building and sustained advocacy can knock a place onto a different path, sometimes faster than the blink of an eye.
During Amy Coney Barrett’s Supreme Court hearing, former U.S. Senator Dianne Feinstein referenced coat hangers and trips to Mexico in the pre-Roe world. This new world looks different- it’s aided by pills and strangers and operates in secrecy, but also on the ballot in the minds of a generation who thought these worries were a relic of the before times. This may be the biggest shift post-Dobbs — a radical shift in ontologies, in being reminded that the infrastructure and legal cocoon of rights around you is incredibly fragile and that as soon as you step over an invisible border, it can morph into a vehicle for punishment, shame, a moral panic, or another sad story. As technical and boring as “considering the spatial dimensions of policy” sounds, it’s critical to making choices that affect change within communities — the definition and power of the plan. I don’t take my abortion for granted, but it’s expanded into a watershed of seeing myself as a political actor, a data point, a voice speaking out, and a member of a legal and spatial capital “P” place where my personhood is affirmed. In going through the process of an abortion and feeling zero regrets, one realizes how personal the whole experience is, despite layers and layers of agitprop telling you how you’ll feel. The outcomes are mine and mine alone to experience, and that freedom in knowing what my future will look like is profound.
Note: I use “women” in this piece for clarity, but I would like readers to know that everyone’s- regardless of gender identity or reproductive parts setup, so to speak- access to affirming health care is paramount. Abortion care recipients span identities, and those who fall outside of cis, straight womanhood face intersecting challenges.
Brittany Jeffery is a Master of Urban Planning Candidate whose current interests lie at the intersections of public health, policy, and spatial planning. One of the few artists residing in Brooklyn, NY (haha), she is drawn to both words and the visual realm as she continues a lifelong investigation of how to convey feelings and meaning in the graphic space.